
Case: A young woman with chronic nasolacrimal duct obstruction presents with 5 days of right sided swelling around her right eye. She was prescribed oral antibiotics by her primary care doctor, but symptoms worsened despite taking them. She denies systemic malaise, fevers, chills, rigors. She can see normally out of both eyes. No pain with eye movement, no photophobia. On exam, you notice soft swelling and erythema around the eye with scant mucopurulent discharge coming from the nasolacrimal duct associated with firm swelling and extreme tenderness of the nasolacrimal duct region medial and below the eye. Extraocular movements are intact bilaterally, and no relative afferent pupillary defect is present.
Question: What is the clinical diagnosis and treatment?
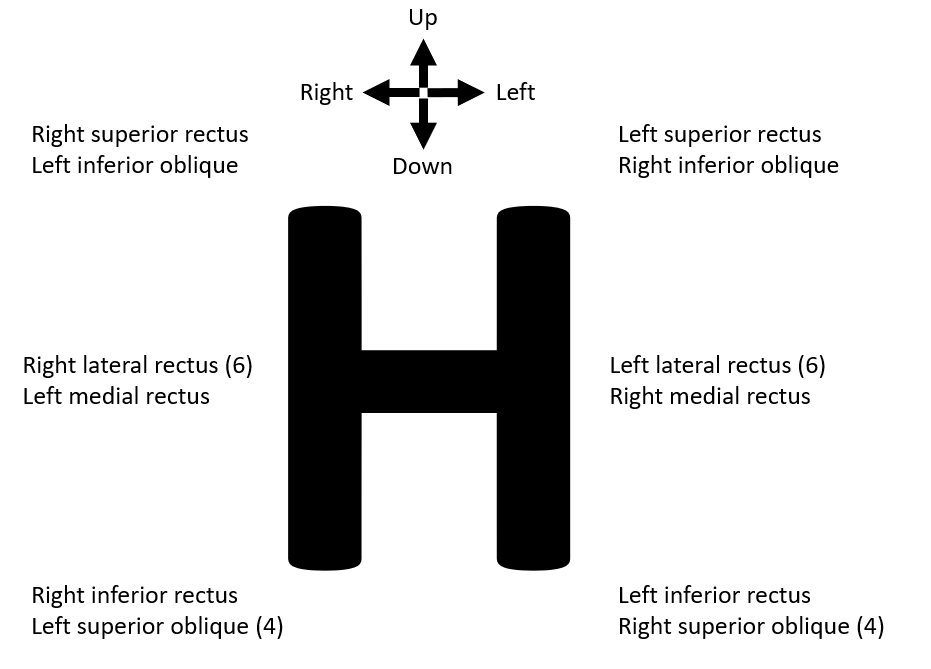
Answer: Acute dacrocystitis with preseptal cellulitis. The patient has acute dacrocystitis which is an acute infection in the setting of chronic nasolacrimal duct obstruction. The most common causative pathogens in adults include Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pneumoniae, and Pseudomonas aeruginosa. Treatment involves warm compresses and systemic antimicrobials, typically PO agents covering Gram positive pathogens, but if the clinical presentation is severe or the patient is not improving, then broader IV antimicrobials should be used. Potential complications include preseptal cellulitis, as in the case of our patient. Preseptal cellulitis should always be differentiated from orbital cellulitis. Signs of orbital cellulitis (with or without orbital abscess) includes proptosis, pain with eye movement, ophthalmoplegia, and relative afferent pupillary defect (rAPD). Remember to move the eye in all cardinal directions in the shape of an H and to look for a rAPD with the swinging flashlight test (see below). Acute dacrocystitis does not typically cause orbital cellulitis because the nasolacrimal duct is anterior to the orbital septum, but it has been rarely reported in cases of fistulazation into the orbit so obtain orbital imaging and STAT ophthalmology consultation if you have concern for orbital cellulitis. Other complications include nasolacrimal sac abscess, and septic cavernous sinus thrombosis with CNS extension in rare cases.
Definitive treatment involves surgically correcting the nasolacrimal duct obstruction, but this should not be done until acute infection/inflammation has resolved to avoid creating a fistula in inflamed tissues. The definitive procedure for adults is typically called a dacryocystorhinostomy (DCR), performed by an ophthalmologist.
Cardinal eye movements:
References:
https://eyewiki.aao.org/Dacryocystitis
Kikkawa DO, Heinz GW, Martin RT, Nunery WN, Eiseman AS. Orbital Cellulitis and Abscess Secondary to Dacryocystitis. Arch Ophthalmol. 2002;120(8):1096–1099
